Intraventricular Hemorrhage Ken Schroeter,
DO
I. Head
Ultrasound (HUS) Guidelines
Birth Weight Day of Life
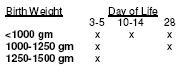
-All infants with a birth weight
<1500 gm get HUS at discharge -Obtain HUS more frequently if pathology
exists
II. Intraventricular
Hemorrhage (IVH). IVH
is an intracranial hemorrhage that originates in the subependymal
germinal matrix, and may extend into the ventricles of the brain, may progress
to dilation of the ventricles, and may include areas of periventricular
white matter infarction. The diagnosis is made by HUS, but more serious cases
(Grade III, IV) are evaluated further with cranial computed tomography or
magnetic resonance imaging. Incidence and severity are inversely related to
gestational age. The highest risk for developing IVH of any grade is in the
first 3 days of life. HUS done in the first 4-7 days of life will detect
90-100% of all IVH.
Grade I Subependymal (germinal matrix) hemorrhage
-Majority resolve completely -88-95% will have normal
neurological outcome
Grade II
IVH without ventricular dilatation (blood in the ventricle)
-Majority resolve completely
-85% will have normal neurological outcome
Grade III
IVH with ventricular dilatation
-65-73% will have a normal neuro
outcome, but associated mortality is 8%
Grade IV
IVH with periventricular hemorrhagic infarction
-86-90% will have major motor
deficits, 64% will have major cognitive problems, and associated mortality
approaches 60%, especially < 1.5 kg
Periventricular Leukomalacia (PVL)
-Focal
necrosis of periventricular white matter, dorsal and
lateral to the ventricles,ischemic
(not hemorrhagic). Large cysts form in severe PVL. 25-40% of
preterm infantsaffected. It is not caused by
IVH, but frequently associated with it.-HUS not as sensitive, CT/MRI not
initially helpful-Cystic formation is associated with poorer neurologic outcome.-82% of children with cerebral palsy
have PVL. Most with PVL will have someneurocognitive
disorder such as attention disorders, learning disabilities, and subtlebehavior problems.
Examples
of Head Ultrasounds
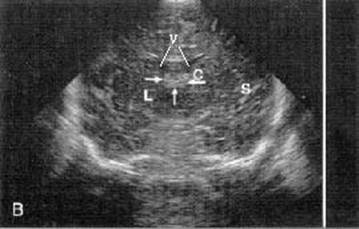
Normal Coronal HUS. V: lateral ventricles, C: caudate head, Arrows: choroid
plexus,
L: lentiform nucleus, S: Sylvian
fissure.
Normal Sagittal
HUS. V: Ventricle, C: Caudate, T:
Thalamus, Arrows: Caudothalamic groove.

Grade I Subependymal hemorrhage (sagittal view).

Grade II extension into the ventricle (sagittal
view).

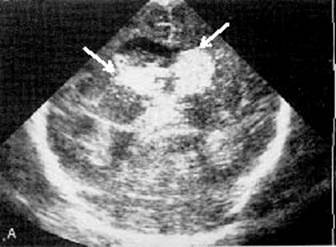
Grade III extension with dilatation (coronal view).
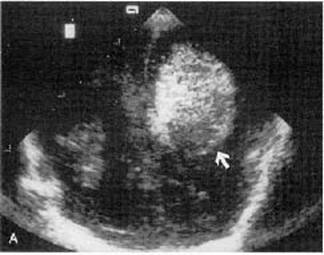
Grade IV Periventricular infarction (coronal view)
Ref: Bulas, D and Vezina, G, Preterm
Anoxic Injury -Radiologic evaluation, NeonatalImaging, Radiologic
Clinics of North America, Volume 37, Number 6, November 1999